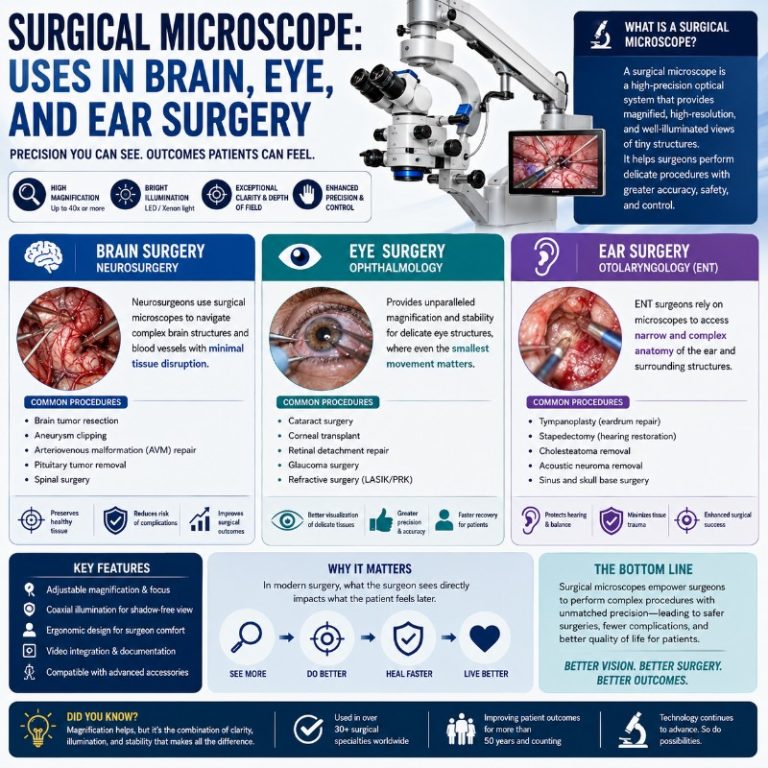
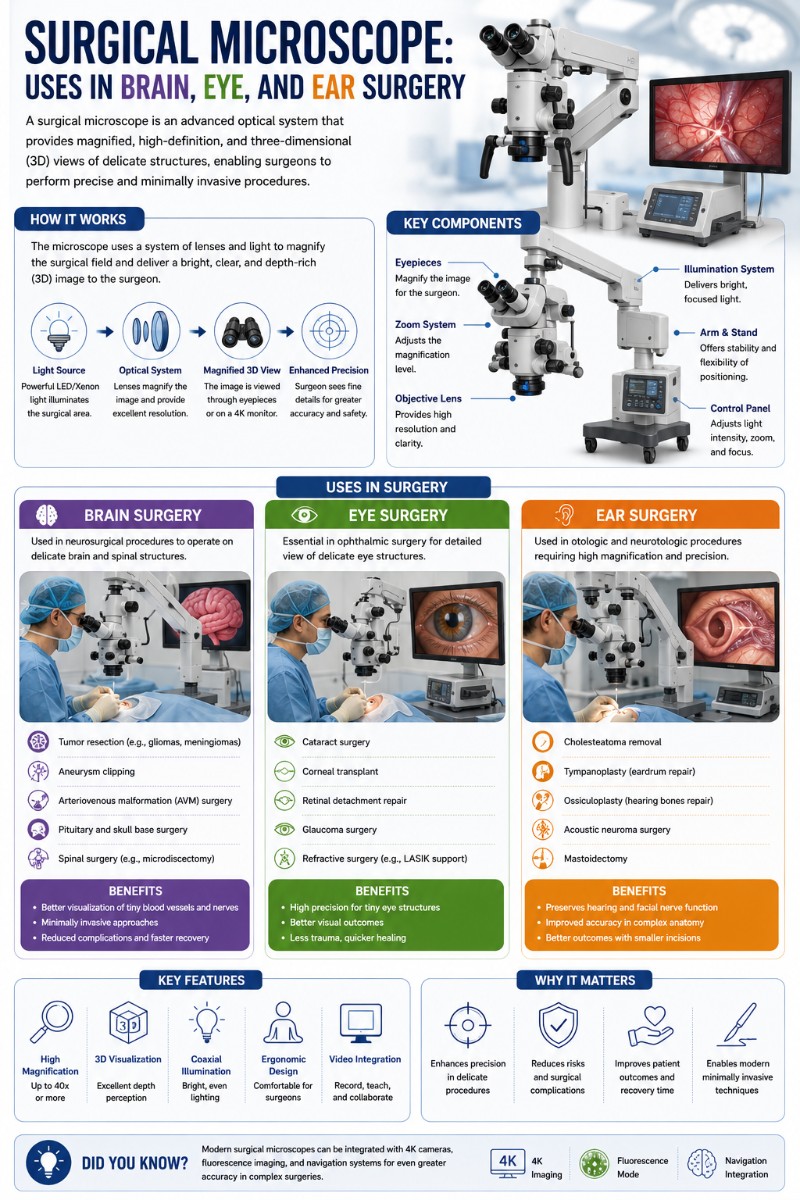
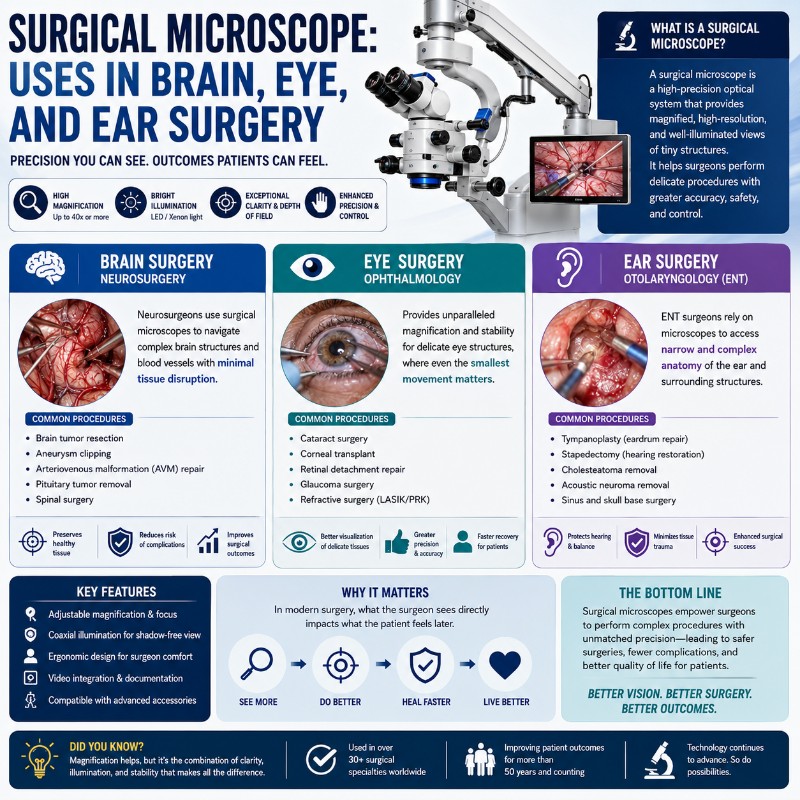
A surgical microscope — also called an operating microscope — is a binocular stereo microscope mounted on a counterbalanced stand that gives surgeons a magnified, brilliantly lit, three-dimensional view of the operative field. Unlike the high-powered compound scopes used in a biology lab, it operates at modest magnification (roughly 4× to 40×) with a working distance of 200–400 mm, leaving enough room for hands and instruments. Neurosurgeons, ophthalmologists, ENT specialists, dentists, and microsurgeons all depend on it — the same core instrument adapted to entirely different anatomies. This article is an educational overview of different types of microscopes that surgeons use; it is not medical or surgical guidance.
How a Surgical Microscope Differs From a Lab Microscope
Most people picture a compound microscope when they hear the word “microscope” — the upright instrument with a condenser below the stage and a 40×–1,000× magnification range. A surgical microscope shares only the lens glass. In design, purpose, and optics it is a fundamentally different instrument. Understanding those differences is the fastest way to understand why surgeons need one at all.

| Feature | Surgical (Operating) Microscope | Compound (Lab) Microscope |
|---|---|---|
| Magnification range | ~4× – 40× (working range 6× – 25×) | 40× – 1,000× (or higher) |
| Working distance | 200 – 400 mm (objective to field) | A few millimeters |
| Illumination | Coaxial (down the optical axis, no shadows) | Transmitted (condenser below stage) or reflected from above |
| Optical path | Two separate paths → true stereoscopic 3D | One optical path split to two eyepieces — no real depth |
| Image orientation | Erect (right-way-up, uninverted) | Inverted |
| Mount | Articulated floor/ceiling stand, counterbalanced | Fixed bench stand |
Long Working Distance and Low Magnification
The most counterintuitive fact about a surgical microscope is that it deliberately uses low magnification. Surgeons typically operate in the 6× – 25× range. Push the magnification higher and three bad things happen simultaneously: the field of view shrinks, the image darkens, and the shallow depth of field becomes razor-thin — sometimes less than a millimeter in focus at once. A surgeon needs a wide, bright, 3D picture of what’s in front of them, not a tiny, dim, flat one.
The working distance is the other defining feature. An objective lens with a 250 mm focal length holds focus at 250 mm from the field — about 10 inches. That gap is the surgical workspace: hands, instruments, irrigation, suction, and the surgeon’s maneuvering room all live in that 10-inch column of air between lens and patient. A lab compound microscope, by contrast, works at a few millimeters — useful for a glass slide, useless for a live surgical cavity.
One more counterintuitive point worth internalizing: surgeons routinely zoom back down after a close-up look. Starting at low magnification to orient, zooming in for fine work, then zooming back out to re-check context is standard technique. Hobbyists instinctively crank magnification up; experienced surgical observers learn to crank it down.
Coaxial Illumination and Stereo (3D) Vision
Light in a surgical microscope travels down the same optical axis as the surgeon’s view. This coaxial arrangement is what makes the instrument indispensable for deep, narrow cavities. An ear canal, a craniotomy, a root canal — all of these have walls that would cast shadows under any off-axis light source. Coaxial illumination eliminates shadows entirely; tissue looks lit from within, not from the side. Modern sources are LED or xenon for daylight-balanced color rendering, delivered through fiber-optic cables. (This is the complete opposite of a lab microscope’s transmitted-light condenser, which shines up through a transparent specimen from below.)
The second headline feature is stereoscopic depth. The surgical microscope routes light through two physically separate optical paths — one to each eye — creating genuine 3D depth perception. In practice, looking through one for the first time is startling: instruments seem to float in real space, tissue planes have tangible separation, and depth judgment is intuitive rather than inferred. A standard “binocular” lab compound scope splits a single image to two eyepieces; there is no true parallax, and the image is effectively flat. For a surgeon tying a suture to a blood vessel under a millimeter wide, that distinction is the difference between safe and dangerous. Understanding the stereo microscope principle is the key to understanding why surgical scopes work the way they do.
The Stand, Foot Controls, and Co-Observer Ports
A surgical microscope is mounted on a counterbalanced floor stand, ceiling mount, or wall arm, with multiple articulating joints locked by electromagnetic brakes. The counterbalancing means the scope is near-weightless to reposition — nudge it and it stays put. Adjustment during a procedure is handled by foot pedals (and sometimes a mouthswitch), which control zoom, focus, and XY positioning without the surgeon removing their hands from the field or breaking sterile technique.
Built-in beam splitters feed co-observer eyepieces (for an assistant or resident to follow along), a camera for photo and video documentation, and a heads-up display. That documentation capability — real-time HD video of the operative field — is something no surgical loupe can replicate, and it makes the microscope essential for both teaching and medicolegal record-keeping. A quick note on the co-observer port: the assistant’s eyepiece is slightly off-axis, so their view is not identical to the primary surgeon’s. Learning to work with that parallax takes practice, and it’s one of the things that makes teaching on the scope trickier than it looks.

https://www.youtube.com/watch?v=s0t135cwI1c
The Medical Specialties That Rely On It
Because of its combination of coaxial illumination, true 3D depth, and a hands-free zoom, the surgical microscope has become essential across a surprisingly wide range of disciplines — each exploiting a different aspect of its optics.
| Specialty | Primary Uses | Typical Working Magnification |
|---|---|---|
| Neurosurgery | Tumor resection, aneurysm clipping, microvascular decompression | 6× – 25× |
| Ophthalmology | Cataract, corneal transplant, vitreoretinal surgery | 4× – 16× |
| ENT / Otology | Stapedectomy, tympanoplasty, cochlear implant | 6× – 25× |
| Dentistry / Endodontics | Root canal, apicoectomy, fracture detection | 8× – 20× |
| Plastic / Reconstructive | Vessel anastomosis, free-flap transfer, digit replantation | 10× – 25× |
| Spine / Gynecology / Hand | Spinal decompression, tubal reanastomosis, nerve repair | 6× – 16× |
Neurosurgery
Neurosurgery and the operating microscope are so intertwined that modern brain surgery is essentially unimaginable without one. Tumor resection — especially deep-seated gliomas, meningiomas, and acoustic neuromas — requires navigating around critical vessels and nerves at a scale invisible to the naked eye. Aneurysm clipping demands placing a titanium clip on the neck of a bulge in a vessel that may be only 2–3 mm in diameter; the 3D depth of the scope is what lets the surgeon see the clip jaws in true relation to the vessel wall.
Fluorescence-guided surgery has become a major recent advance in neuro-oncology. 5-ALA (aminolevulinic acid, sold as Gleolan and FDA-approved specifically for glioma visualization) is given to the patient before surgery. It accumulates in tumor tissue and fluoresces pink-red under blue-violet light — a filter built into the microscope head. Looking through the scope under fluorescence mode, the glioma glows distinctly against the grey-white surrounding brain. That pink glow is not subtle; it looks like someone switched on a neon light inside the tissue, and it lets surgeons push resection further with more confidence about margins. ICG (indocyanine green) is used similarly for vascular and perfusion imaging, showing blood flow in real time as a bright fluid filling a vessel riverbed.
Ophthalmology
The eye is a closed, fluid-filled sphere roughly 24 mm across. Everything inside it — the lens, the iris, the retina, the vitreous — must be reached through incisions measured in fractions of a millimeter. The surgical microscope provides the coaxial red-reflex illumination that makes cataract surgery possible: light travels down the optical axis, enters the pupil, reflects off the retina, and returns through the pupil as an orange-red glow — the red reflex. The cataract-clouded lens is visible as a grey silhouette against that glow, giving the surgeon the contrast needed to emulsify and remove it safely.
Corneal transplant, glaucoma filtering procedures, and vitreoretinal surgery (detached retina repair, macular hole closure, membrane peeling) all similarly depend on the scope’s combination of bright coaxial illumination, 3D depth, and the fine hand-control that foot-pedal zoom provides. The binocular eyepiece system is especially important here — both eyes are needed for the depth judgment that microinstrument work demands.
ENT and Ear (Otology)
The ear is where the surgical microscope was born, and it remains indispensable in otology. The ear canal is roughly 25 mm long and 7 mm wide — a deep, narrow, dark tube with the eardrum at the end. Coaxial illumination is the only practical way to light it without shadows. A stapedectomy (replacing the tiny stapes bone — about 3 mm long — to treat otosclerosis-related hearing loss) is performed entirely through that canal under 10× – 25× magnification. Tympanoplasty (eardrum repair), cochlear implant surgery, and laryngeal microsurgery (vocal cord work) all rely on the same principle: a deep cavity that can only be properly illuminated and magnified by an operating microscope on a stable counterbalanced stand. Otolaryngology remains one of the highest-volume surgical microscope use cases in any major hospital.
Dentistry and Endodontics
The operating microscope entered dentistry later than medicine — widespread in endodontic (root canal) practices from the 1990s onward — but its impact has been substantial. Root canals branch, curve, and hide. A missed canal, an untreated isthmus, a hairline fracture in the root — these are sources of treatment failure. Many are genuinely invisible to the naked eye or even to loupes. Under 10× – 20× magnification with coaxial light, an endodontist can locate a calcified canal orifice, visualize cracks in root dentin, and perform microsurgical apicoectomy (root-end surgery) with precision impossible by any other means. A dental operating microscope is smaller and lighter than an OR scope, but the optical principles — stereo depth, coaxial light, foot-pedal zoom — are identical.
Plastic and Reconstructive Microsurgery
Microsurgery is the discipline that most directly defines what a surgical microscope makes possible: anastomosing (reconnecting) blood vessels and nerves smaller than 3 mm in diameter. Replanting a severed finger means suturing arteries, veins, and digital nerves under 10× – 25× magnification, placing sutures finer than a human hair. Free-flap transfers — moving a block of tissue with its blood supply from one part of the body to another to reconstruct a mastectomy site, a jaw, or a burned limb — depend entirely on the microsurgeon’s ability to connect vessels 1–2 mm across end-to-end with enough precision that they stay patent. Lymphatic surgery (lymphovenous anastomosis for lymphedema) takes that precision further still, working on channels less than 1 mm across. The surgical microscope is not optional in this specialty; it is the specialty.
Other Fields
Spinal surgery uses the microscope for minimally invasive decompression procedures, allowing surgeons to work through small incisions with less muscle retraction. Gynecological microsurgery — notably tubal reanastomosis (reconnecting fallopian tubes after prior ligation) — relies on it for suturing delicate tube walls back together. Hand surgery (nerve repair, tendon work) and urology (vasovasostomy — vasectomy reversal) round out the picture. The parts of a microscope that make it useful in all these settings are the same: stable mounting, coaxial illumination, foot-controlled zoom, and true stereoscopic depth. The anatomy changes; the optical tool stays the same.
How It Fits Into the Operating Room
A surgical microscope does not simply roll in and get pointed at the patient. Its integration into OR workflow involves careful preparation, and the experienced surgical team treats it as a primary piece of equipment, not an accessory.
Before any case begins, the scope is positioned and balanced — the counterweights adjusted so the head floats effortlessly at any angle. Rebalancing mid-case because setup was rushed is a genuine frustration, and experienced OR teams know to do this before draping. A sterile drape then envelops the scope body, with a clear optical window positioned over the objective. If the drape is tented incorrectly over the lens, it creates glare and degrades the image — a common setup error in teaching institutions.
The surgeon adjusts the eyepiece diopters and interpupillary distance to their own eyes before scrubbing. A mis-set scope gives eyestrain within minutes and destroys the 3D effect — both eyes must be in focus simultaneously for the stereo view to work. Once the case starts, all zoom, focus, and XY repositioning is done by foot pedal, keeping both hands sterile and on the field.
The camera output feeds a monitor in the room — for a scrub tech to follow what the surgeon is doing, for a resident on the co-observer eyepiece to learn in real time, and for recording. The assistant’s co-observer view is slightly off-axis from the primary surgeon’s, which creates a mild parallax — fine for following along, but an adjustment for anyone learning to assist on the scope for the first time. For an educational overview of how optical (light) microscopes like this compare to other microscope types, the contrast with electron microscopy is instructive: everything in surgery operates in the realm of visible light and real-time manipulation.
Where Surgical Microscopes Are Heading
The surgical microscope is not a static technology. Three trends are reshaping what it is and how it’s used, and any reader who wants to understand the state of the field needs to know them.
Fluorescence-guided surgery has already transformed neurosurgery and is expanding across specialties. Beyond 5-ALA for gliomas, ICG fluorescence is used to assess flap perfusion in plastic surgery (is the blood flowing through the transferred tissue?), to check anastomosis integrity (is the vessel actually patent?), and to map sentinel lymph nodes. These fluorescence modes are now built into high-end surgical microscopes as toggle-able filter sets rather than add-ons.
Digital “exoscopes” are the most disruptive development in surgical optics in decades. Instead of the surgeon looking through optical eyepieces, a high-definition camera on a long arm captures the field and displays it on a 4K or 3D monitor in the OR — a setup called “heads-up surgery.” The ergonomic case is compelling: surgeons working through eyepieces often crane their necks for hours at a stretch, leading to cervical spine problems that are nearly endemic in neurosurgeons and otolaryngologists. Looking at a monitor in a natural head position eliminates that strain. Examples include the Zeiss KINEVO 900 (a hybrid scope/exoscope), the Olympus ORBEYE, and the Synaptive Modus V. The tradeoff is that true stereoscopic depth requires either passive 3D monitors (with polarized glasses) or active shutter systems — standard 4K is effectively flat — and the tactile-visual coupling of looking directly through optics is different from using a screen.
Robotic and digitally-assisted positioning is the third frontier: motorized arms that hold position without drift, image-injection systems that overlay a navigation MRI onto the live scope image, and in some cases semi-automated repositioning integrated with surgical navigation systems. The underlying magnification versus resolution trade-offs haven’t changed, but digital processing is beginning to extend what surgeons can perceive through the scope in real time.
Frequently Asked Questions
What is a surgical microscope called?
The formal generic name is operating microscope. The abbreviation OPMI — which stands for “Operating Microscope” — originated as a Zeiss product line name when the company released the OPMI 1 in 1953, and it became widespread shorthand in surgical circles. You may also hear it called a surgical microscope, surgical operating microscope, or simply “the scope.”
Who invented the surgical microscope, and when?
Swedish otologist Carl-Olof Nylén built the first surgical microscope in 1921 — a modified monocular lab scope adapted for ear surgery. His colleague Gunnar Holmgren added illumination and developed a binocular version in 1922. The first commercially produced operating microscope, the Zeiss OPMI 1, was released in 1953 and made the instrument available to hospitals worldwide. For more context, the history of the microscope traces how these instruments evolved across centuries.
How much does a surgical microscope cost?
New high-end surgical microscopes from manufacturers like Zeiss, Leica, and Olympus typically range from $50,000 to over $500,000, depending on the optical configuration, digital integration, fluorescence modules, and mounting system. Entry-level dental operating microscopes can be found for $5,000–$20,000. Refurbished units are widely available and significantly less expensive.
What is the difference between a surgical microscope and surgical loupes?
Surgical loupes are lightweight magnifying lenses worn like glasses or mounted on a headband, typically providing 2× – 6× fixed magnification. They are inexpensive, portable, and require no setup, but they cannot zoom, have limited illumination (a separate headlight is attached), provide no documentation, and top out at magnification levels too low for many procedures. A surgical microscope offers variable zoom up to ~40×, far greater illumination intensity, a camera feed, co-observer ports, and true stereo depth — at the cost of setup time, a large footprint, and significantly higher price.
What is an exoscope, and how is it different from a surgical microscope?
An exoscope is a camera mounted on a rigid or robotic arm that projects the surgical field onto a high-definition monitor — the surgeon views a screen rather than looking through eyepieces. It eliminates the physical eyepiece entirely. A traditional surgical microscope relies on the surgeon’s eyes at the optical endpoint of a lens system. Exoscopes offer better ergonomics (natural head position, no neck craning) and easier room-wide visualization, but achieving true 3D depth requires specialized 3D display systems. The two categories are converging in hybrid devices like the Zeiss KINEVO.
Can a surgical microscope transmit infection?
The scope body is never sterile — it is covered by a sterile drape for each case. The optical objective, co-observer ports, and camera connections are all draped or covered with sterile barriers before use. Proper draping technique is a required skill in surgical training, and hospitals have protocols specifying exactly how each scope model is covered and cleaned between cases.
Why does the surgeon sometimes zoom out during surgery?
Counter-intuitively, high magnification is not always better. At high zoom, the field of view is small, the image is darker, and the depth of field is a fraction of a millimeter — the slightest movement throws tissue out of focus. Surgeons routinely zoom back out to re-orient (confirm where they are in the anatomy) and to work at a magnification where the field is wide enough to operate efficiently. The skill is in knowing when to zoom in for precision and when to pull back for context.
Conclusion
The surgical microscope is, at its core, a low-magnification stereo microscope with coaxial illumination, a long working distance, and a counterbalanced stand built for the operating room. Those design choices — modest magnification, shadow-free light, hands-free control, and true 3D depth — are what make it indispensable from the delicate bones of the ear to the vessels of the brain, from a root canal to a replanted finger. Understanding the stereo microscope principle behind it explains why the instrument works so differently from the compound scopes most people encounter in a science class, and why fluorescence-guided and heads-up systems represent genuine extensions of the same core idea rather than replacements for it.
Have you ever observed a procedure through a surgical microscope — in person, through a co-observer port, or on video? Or are you a student or professional curious about a specialty we covered here? Tell us what you found (or what you’re wondering about) in the comments below.